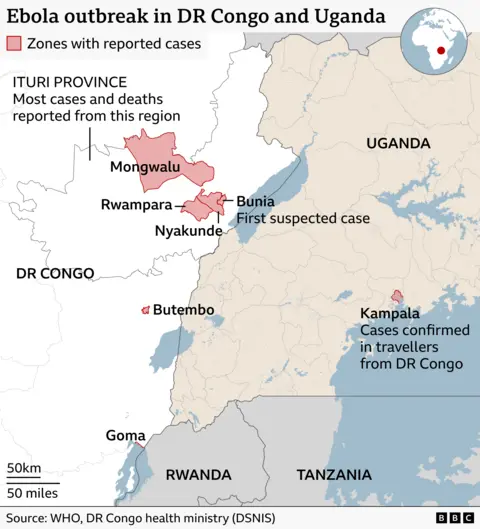
The World Health Organization is now tracking 139 suspected deaths and 600 Ebola cases in an active outbreak — and the agency has warned that a vaccine will not be available for deployment for at least nine months. Nine months. That is not a supply chain delay. That is the consequence of what happens when the world's early-warning and rapid-response architecture is stripped down to its studs and left to rust.
The BBC reported the WHO's latest figures, but the more important number is not in the case count. It is the gap between when an outbreak like this becomes detectable and when the international system is capable of responding to it. That gap used to be smaller. It was made smaller, deliberately, over two decades of investment in global health infrastructure — surveillance networks, pre-positioned medical supplies, trained local responders, coordinated logistics. Much of that investment flowed through USAID. Most of that investment is now gone.
Earlier this year, the Trump administration effectively dismantled USAID, the agency that for decades served as the operational backbone of American global health engagement. This was not a budget trim. Programs that took years to build — field epidemiology training, laboratory capacity in outbreak-prone regions, community health worker networks — were cut with no transition plan and no successor system. The people who knew how to run those programs were fired. The institutional memory walked out the door with them.
The nine-month vaccine timeline deserves scrutiny on its own terms. Ebola is not a new disease. The first outbreak was documented in 1976. There have been dozens since. A vaccine — rVSV-ZEBOV, marketed as Ervebo — was approved by the FDA in 2019 and has been used in ring vaccination campaigns in the Democratic Republic of Congo. The fact that a vaccine cannot be deployed for nine months in a 2025 outbreak is not a scientific failure. It is a logistical and political one. Getting a vaccine from a cold-storage facility to the people who need it requires functional health systems, trained vaccinators, community trust networks, and coordination infrastructure. These are exactly the things that USAID funding helped maintain in the regions most at risk.
The accountability question here is not abstract. Specific decisions, made by specific people, created the conditions in which this outbreak is now spreading without an adequate international response. The Office of Management and Budget approved the USAID cuts. The Department of Government Efficiency, operating without congressional authorization, executed them. The administration framed the cuts as eliminating waste. What they eliminated was the institutional capacity to do what wealthy countries always promise to do in a pandemic: catch it early, contain it fast, and get medicine to people before the death toll climbs into the hundreds.
USAID's global health programs included the Global Health Security Agenda, which built laboratory networks and trained field epidemiologists in outbreak-prone countries. The agency also funded the Emerging Pandemic Threats program, which operated in more than 30 countries to detect and contain novel pathogens. These programs were defunded or dismantled in the early months of 2025. No replacement architecture has been announced.
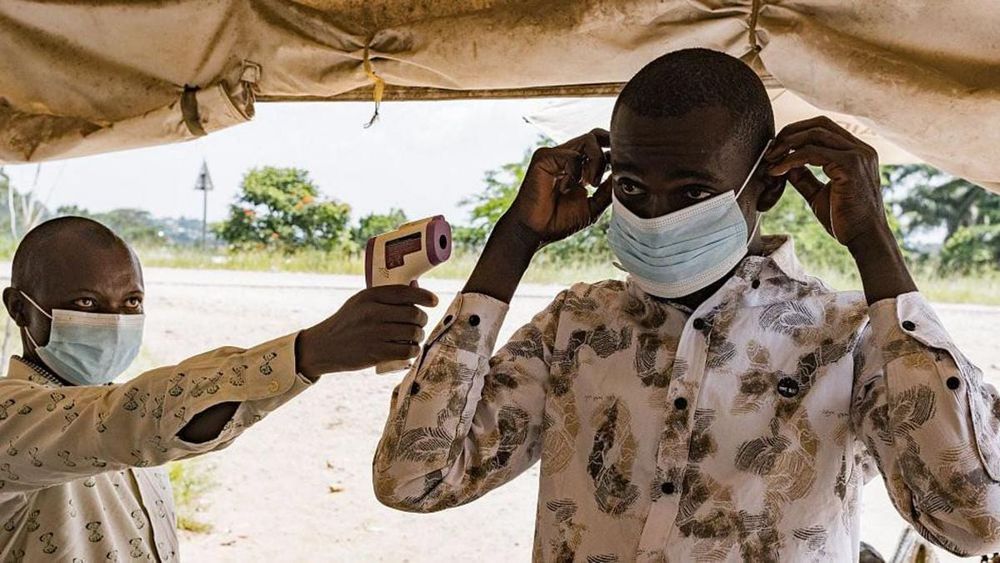
This is also a story about whose suffering gets counted as urgent. Ebola outbreaks have historically occurred in Central and West Africa — in the Democratic Republic of Congo, Guinea, Sierra Leone, Liberia. The disease kills quickly and visibly. It generates photographs that run on international news sites for a week, then disappears from the coverage cycle until the death toll forces it back. The communities bearing this outbreak are not the communities whose governments are making the decisions about global health funding. That asymmetry is not incidental. It is the structure.

The WHO has issued its warning. The case count is climbing. The vaccine timeline is what it is. But the question the BBC's report does not ask — and the one this outbreak demands — is who decided that the infrastructure preventing exactly this scenario was expendable. The answer is documented. It is in the executive orders, the budget memos, the DOGE directives that shut down USAID programs country by country in the first weeks of 2025. The people who made those decisions are not in the affected region. They will not be.
Critics of the cuts, including global health policy experts and former USAID officials, have argued consistently that the dismantling of the agency's health security programs would not save money in any meaningful long-term sense — that the cost of responding to outbreaks that early-warning systems fail to catch is orders of magnitude higher than the cost of the systems themselves. The 2014-2016 West Africa Ebola epidemic, which killed more than 11,000 people and cost an estimated $53 billion in economic losses across affected countries, is the standard reference point. The global response to that outbreak was slow, under-resourced, and dependent on exactly the kind of international coordination infrastructure that has since been hollowed out.
There is also a domestic dimension that the framing of this as a "foreign" crisis obscures. Infectious disease does not observe the jurisdictional logic of aid budgets. The COVID-19 pandemic demonstrated, at catastrophic cost, that an outbreak that begins in one country and is not contained quickly does not stay in one country. The global health security infrastructure that USAID helped fund was not charity. It was, as public health professionals have argued for years, early intervention at a fraction of the cost of late response. The hollowing out of health systems — whether domestic or international — does not reduce the burden of disease. It defers it, and compounds it.
The WHO's nine-month vaccine estimate is the kind of figure that sounds like a logistical detail and is actually a verdict. It is a verdict on what the world chose to invest in and what it chose to defund. A functioning rapid-response system — the kind that USAID programs spent two decades helping to build — does not produce a nine-month gap between outbreak and vaccine deployment. It produces weeks. The gap between weeks and nine months is not a gap in science. It is a gap in political will, filled in by budget decisions that were made in Washington and are now being paid for by people in a region that had no vote in those decisions.
As this outbreak grows, the international community will convene meetings, issue statements, and eventually mobilize a response. That response will be slower, more expensive, and less effective than it would have been if the infrastructure dismantled earlier this year were still intact. The warning signs were visible before this outbreak began. The people responsible for dismantling the systems that should have caught it earlier are not being asked to account for the nine months — or the 139 people already dead.



